





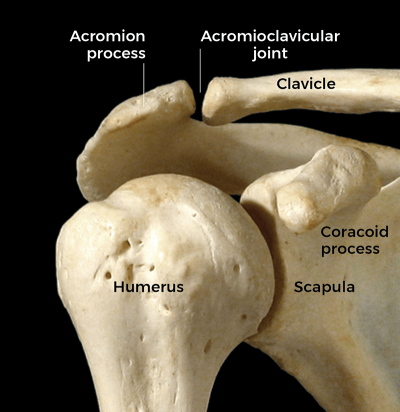
When working with clients who have a shoulder condition, our first thought might be to assess and treat the myofascial tissues across the glenohumeral (GH) joint (Image 1). The deltoid and rotator cuff muscles might spring to mind.
The idea that there is a coupling of movements between the arm at the GH joint and the shoulder girdle relative to the trunk is called scapulohumeral rhythm.
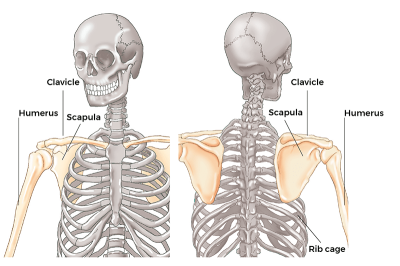
In other words, there is a rhythm between movements of the scapula and the humerus. Even though this term is excellent in that it expands our view of the functioning of the shoulder, it actually is not expansive enough. A better term for this coupled rhythm would be claviculoscapulohumeral rhythm because the clavicle also plays a crucial role in shoulder movement (Image 2). In fact, movement of the clavicle at the sternoclavicular joint may be the most underappreciated motion of the human body.
To better understand the concept of scapulohumeral rhythm, we need to appreciate the fact that the primary purpose of the upper extremity is to place the hand in the positions necessary to work with and manipulate the world. Therefore, whatever joint motions are necessary to accomplish hand placement will work in concert toward this end.
Humerus Coupling with the Scapula
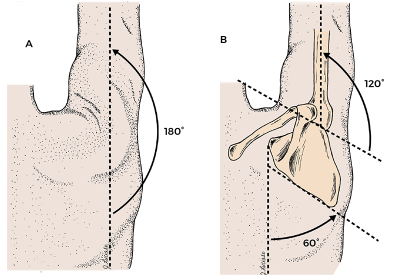
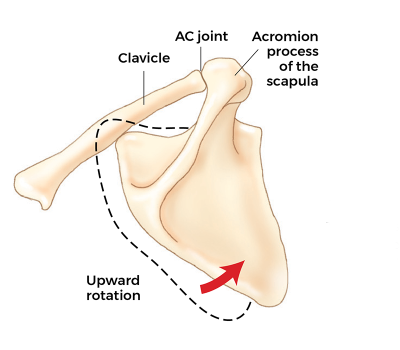
The best example of scapulohumeral coupling of motions is probably frontal-plane abduction of the arm. It is usually stated that the arm can abduct 180 degrees so that the arm is straight up in the air (Image 3A). However, the GH joint does not allow for 180 degrees of abduction. The GH joint itself allows only 120 degrees of humeral abduction, only two-thirds of the 180 degrees that is stated as full arm abduction. The other 60 degrees, the other one-third of this motion, is actually generated by upward rotation of the scapula relative to the rib cage of the thoracic body wall at the scapulocostal (ScC) joint (also known as the scapulothoracic joint). Upward rotation of the scapula is a movement of the scapula at the ScC joint relative to the rib cage such that the glenoid fossa of the scapula orients upward. This affords the head of the humerus the ability to continue rolling upward until the arm is vertical at 180 degrees relative to the trunk of the body (Image 3B).
So, we see that movement of the arm/humerus is strongly dependent upon coupled movement of the scapula. But, as we have mentioned, the clavicle must be included in this conversation as well. There is a rhythm between scapular movement and clavicular movement. In fact, much of the movement of the scapula at the ScC joint is driven by movement of the clavicle. In our example of scapular upward rotation of 60 degrees to accompany full humeral abduction, half of that scapular upward rotation occurs because the clavicle elevates at the sternoclavicular (SC) joint relative to the sternum, and as the clavicle elevates, the scapula is brought along with it such that it changes its position relative to the rib cage. We could say that the scapula passively “goes along for the ride.”
So, even though there are muscles that can actively move the scapula into upward rotation, the scapula can also be passively moved into upward rotation by accompanying elevation of the clavicle. For example, during the first 90 degrees of arm abduction, 60 degrees are due to GH joint humeral motion, and 30 degrees would be due to scapular upward rotation at the ScC joint.
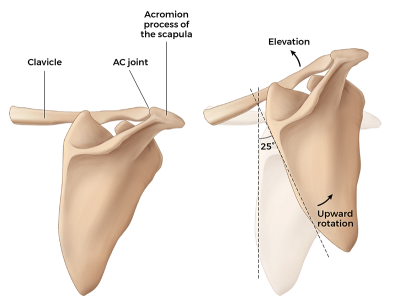
Of these 30 degrees of scapular upward rotation, 25 degrees occur as the scapula is passively moved by clavicular motion (Image 4A). There are another 5 degrees of scapular upward rotation created by the scapula actively upwardly rotating relative to the clavicle at the acromioclavicular (AC) joint (Image 4B) (see "Scaption" sidebar and Image 5 below).
So, the question might be: Is this just anatomy geek information, or is there an application for manual therapists and movement professionals? To answer this question, let’s look at a potential case study.
When we appreciate the concept of scapulohumeral rhythm, our ability to appreciate larger kinematic chains of motion increases.
Potential Case Study
A client presents with decreased abduction range of motion of the right arm. How do we perform our assessment? If we believe that all arm abduction is generated at the GH joint, then we might come to four conclusions:
- There is dysfunction of the GH joint.
- Humeral abductors are weak.
- Humeral adductors (the antagonists of the motion) are tight (hypertonic/overly facilitated/locked short).
- Some other GH joint fascial/ligamentous tissue, including its joint capsule, is taut.
This analysis might lead us toward a physical assessment of the GH joint and its myofascial tissues. However, when we broaden our scope to include scapular and clavicular motion, we realize we need to broaden the scope of our physical assessment as well.
With this broader view of shoulder function in mind, our physical assessment might expand to include the following:
- Palpation and strength assessment of all muscles of humeral abduction, including the deltoid, supraspinatus, biceps brachii long head, and pectoralis major clavicular head.
- Palpation of all muscles of humeral adduction, including the pectoralis major, latissimus dorsi, teres major, coracobrachialis, biceps brachii short head, triceps brachii long head, and teres minor.
- Palpation and strength assessment of all muscles of scapular upward rotation, including the upper trapezius, lower trapezius, serratus anterior, and teres major.
- Palpation of all muscles of scapular downward rotation, including the rhomboids, pectoralis minor, levator scapulae, and deltoid.
- Palpation and strength assessment of all muscles of clavicular elevation, including the upper trapezius.
- Palpation of all muscles of clavicular depression, including the subclavius, anterior deltoid, and pectoralis major clavicular head.
- Motion palpation of the GH, ScC, SC, and AC joints.
- Palpation of all fascial tissues of the GH, ScC, SC, and AC joints.
- The foregoing was a discussion of scapulohumeral rhythm regarding humeral abduction. But scapulohumeral rhythm exists for all six cardinal-plane ranges of motion of the arm at the GH joint. Following is a brief explanation of these six scapulohumeral rhythms.*
- Humeral abduction couples with scapular upward rotation.
- Humeral adduction couples with scapular downward rotation.
- Humeral flexion couples with scapular upward rotation and protraction.
- Humeral extension couples with scapular downward rotation and retraction.
- Humeral lateral rotation couples with scapular retraction.
- Humeral medial rotation couples with scapular protraction.
*Scapular upward and downward rotation couple with clavicular upward and downward rotation respectively; scapular protraction and retraction couple with clavicular protraction and retraction respectively.
When we appreciate the concept of scapulohumeral rhythm, our ability to appreciate larger kinematic chains of motion increases. And along with this, so does our appreciation and competency of how to counsel, assess, and treat our clients not only for shoulder problems, but for all myofascioskeletal conditions of the body.
A Deeper Dive—Scapulohumeral Rhythm: Abduction of the Arm
"Scapulohumeral-rhythm motion of the coupled joint actions of the shoulder joint complex that accompany frontal-plane abduction of the arm at the glenohumeral (GH) joint has been extensively studied. Following is a summation of these complex coupled actions. This level of detail is presented to manifest the beautiful complexity of scapulohumeral rhythm and illustrate the need for a larger, more global assessment of shoulder joint motion in clients who have shoulder problems.
To reiterate, full frontal plane abduction of the arm is considered to be 180 degrees of arm motion relative to the trunk. Of that motion, the arm abducts 120 degrees at the GH joint, and the scapula upwardly rotates 60 degrees at the scapulocostal (ScC) joint (with the arm “going along for the ride”); 120 degrees plus 60 degrees equals 180 degrees of total arm movement relative to the trunk. This total movement pattern can be divided into an early phase and a late phase, each one consisting of 90 degrees."
Early Phase (Initial 90 Degrees):
- During the early phase, the arm abducts 60 degrees at the GH joint and the scapula upwardly rotates 30 degrees at the ScC joint.
- This scapular upward rotation of 30 degrees relative to the rib cage is created by two motions:
- The clavicle elevates at the sternoclavicular (SC) joint, and the scapula goes along for the ride, thus changing its position and upwardly rotating 25 degrees relative to the rib cage at the ScC joint.
- The scapula upwardly rotates 5 degrees at the acromioclavicular (AC) joint relative to the clavicle, again changing its position and upwardly rotating relative to the rib cage at the ScC joint.
Late Phase (Final 90 Degrees):
- During the late phase, the arm abducts another 60 degrees at the GH joint and the scapula upwardly rotates another 30 degrees at the ScC joint.
- This scapular upward rotation of 30 degrees relative to the rib cage is created by two motions:
- The clavicle further elevates at the SC joint and the scapula goes along for the ride, upwardly rotating an additional 5 degrees relative to the rib cage at the ScC joint.
- The scapula upwardly rotates another 25 degrees at the AC joint relative to the clavicle, again changing its position and upwardly rotating relative to the rib cage at the ScC joint.
Summation of Early and Late Phases
- The arm has abducted at the GH joint relative to the scapula 120 degrees.
- The scapula has upwardly rotated at the ScC joint relative to the rib cage 60 degrees.
- This scapular upward rotation relative to the rib cage at the ScC joint is composed of 30 degrees of elevation of the clavicle at the SC joint and 30 degrees of upward rotation of the scapula at the AC joint.
How and Why These Motions of the Scapula Occur
The scapula and clavicle are linked together at the AC joint as the shoulder girdle. Hence, muscular contraction that pulls and moves one bone of the shoulder girdle tends to result in movement of the entire shoulder girdle. Therefore, muscles that pull and cause upward rotation of the scapula tend to also pull the clavicle into elevation; conversely, muscles that pull the clavicle into elevation also result in the scapula upwardly rotating.
Early Phase
- The force of muscular contraction (by scapular upward rotators and clavicular elevators) results in elevation of the clavicle at the SC joint relative to the sternum (25 degrees); by simply passively going along for the ride, the scapula succeeds in upwardly rotating relative to the rib cage (i.e., at the ScC joint). The clavicle elevates until it encounters resistance to this motion by the costoclavicular ligament becoming taut, which limits further motion.
- Once the costoclavicular ligament becomes taut because the clavicle cannot elevate further, the force of the scapular upward rotation musculature continues to pull on the scapula and results in upward rotation of the scapula relative to the clavicle at the AC joint (5 degrees). The scapula upwardly rotates at the AC joint until the coracoclavicular ligament becomes taut, which limits further motion.
- The muscles of upward rotation of the scapula continue to pull on the scapula. However, the clavicle cannot elevate any further at the SC joint, and the scapula cannot upwardly rotate any further at the AC joint.
Late Phase
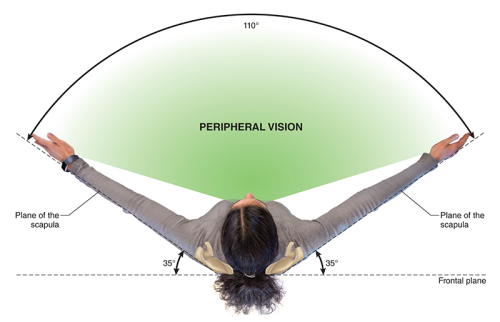
- This continued pull of the scapular upward rotation musculature creates a pull on the scapula that creates tension on the coracoclavicular ligaments. This tension of the coracoclavicular ligaments then pulls on the clavicle in such a way that the clavicle is pulled into upward rotation at the SC joint (the clavicle upwardly rotates approximately 35 degrees).
- Once the clavicle is upwardly rotated at the SC joint, the clavicle can now elevate an additional 5 degrees at the SC joint (because the costoclavicular ligament was slackened) and, more important, the scapula can now upwardly rotate at the AC joint another 25 degrees.
Conclusion
It can be seen that abduction of the arm in the frontal plane is strongly dependent on scapular movement, thus the importance of the term scapulohumeral rhythm. However, it is just as clear that the scapular motion of upward rotation is strongly dependent on clavicular motion, thus the importance of amending the term to claviculo-scapulo-humeral rhythm. Therefore, in assessment of a client with limited frontal plane motion of the arm, it is crucially important to assess not just GH joint motion but also ScC joint motion; assessing ScC joint motion then necessitates assessment of SC and AC joint motion as well. Thus, a case study of frontal-plane arm abduction truly manifests the need for healthy coordinated functioning of all components of the shoulder joint complex.



