





When our bodies are chronically injured or declining, one way of protecting ourselves is to tighten our muscular systems. Prolonged tightening combined with gravitational exposure may lead to inefficient movement and slumping. There are many massage modalities that help improve posture by relieving spasticity in tight, facilitated muscles and activating tone in neurologically weakened muscles. Graded exposure stretching using contract-relax techniques is one of the more popular ways to address muscular imbalance problems via reciprocal innervation. However, in many cases the therapist may need to manually stimulate tone in chronically weakened or atrophied muscles, particularly in clients suffering sensory motor amnesia, where there is a brain-body disconnect. To this end, a myoskeletal technique I call “Spindle-Stim” can be a valuable tool.
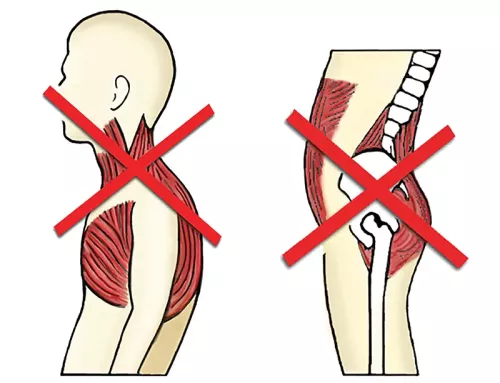
I’ve found this fast-paced spindle-stimulating maneuver particularly effective when treating clients with postural ergonomic stress, as seen in Dr. Vladimir Janda’s upper- and lower-crossed syndromes (Image 1). Janda’s cross syndrome patterns may generally be described as weakening and lengthening of posterior chain muscles, such as the rhomboids, serratus anterior, and gluteals, and tightening and shortening of opposing anterior muscles, such as the pectorals and iliopsoas. Janda’s cross syndromes are not clinically flawless, but they do offer a simplified road map to aid us in assessing weak postures that, left untreated, may lead to chronic neck and back pain.
Clients develop these syndromes for many reasons—from prolonged sitting to midbrain hardwiring issues. Even the memory of an injury and the pain associated with it can cause the body to behave as though it was still injured. This locks the client into the very posture that afforded them avoidance at the time. Likewise, those engaged in job-related sustained or repetitive postures develop muscular imbalances seen in my clinic every day. Before using Spindle-Stim to address such issues, it helps to understand the neurology of this muscle spindle stimulation technique. From there, you can begin to assess, treat, and reassess to determine whether the therapeutic intervention has helped.
Muscle Spindles and the Stretch Reflex
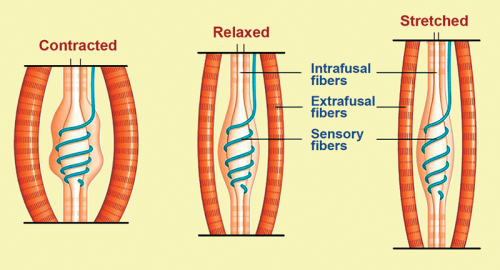
Muscles are recruited through the activation of spindle cells, which are stretch receptors housed within the muscle belly. As the muscle is loaded, the muscle spindle stretches to match the extent of the load. The spindle then sends a signal to the spinal cord, which commands the same muscle to contract. Recall that the contractile tissues within a muscle that generate skeletal movement are called extrafusal fibers, and the intrafusal fibers have the important task of maintaining a smooth length-tension balance with the extrafusal fibers (Image 2). With this in mind, we’re equipped to begin the assessment and treatment steps of Spindle-Stim.
For the assessment, I typically begin by asking the client to perform specific active movement tests, making note of any range-of-motion restrictions (Images 3 and 4). Testing side to side, if I discover a muscle group that appears to have a weak firing pattern, I log the information in my SOAP notes, treat the area, then reassess. The treatment itself focuses on using soft fingers, fists, or forearms to create a rapid length change in the agonist muscle’s extrafusal fibers (Images 5 and 6). This, in turn, stimulates intense firing of the intrafusal fibers, which are valiantly trying to maintain a constant length-tension relationship with the muscle being stretched.

By moving in all directions across the muscle belly, the Spindle-Stim maneuver triggers a mild stretch reflex that helps protect the muscle from injury. I’ve found that stimulating this stretch reflex not only aids in strengthening the weak agonist muscles by restoring resting tone, but also facilitates improved communication between the inhibited muscle and the client’s nervous system. In the beginning, this fast stretch produces a relatively short-lived contraction of the agonist muscle and inhibition of the antagonist muscle. However, over a series of sessions, these effects appear to last longer, particularly when clustered with graded exposure stretching techniques and specific home retraining advice.
Notice in the Spindle-Stim technique descriptions (Images 5 and 6) that I also make use of movement enhancers, such as forced inhalation-exhalation and slow pelvic-tilting maneuvers, to boost the therapeutic effect. Instead of focusing on getting the tight muscles to relax, the idea here is to persuade the weak muscles to tighten and contract properly. This increases joint stability by reciprocally relaxing the hypercontracted spastic muscle, thus affording better overall muscle balance.


Breaking the Cycle
Failure of the smooth self-regulating function of the muscle’s sensory receptors may result in a catch-22 cycle, as faulty postural alignment initiates righting reflexes that trigger muscle spasm and mechanically alter spinal joint motion. As hyperexcited joint and ligament mechanoreceptors initiate protective splinting, some muscles overwork and others become neurologically inhibited, as seen in Janda’s cross syndromes. This results in reduced mobility, excessive energy consumption, exhaustion, and—if the brain perceives threat—pain.
In an effort to break this dysfunctional cycle and help clients heal, try the Spindle-Stim technique coupled with graded exposure stretching and an appropriate home retraining plan.


