





The carpal tunnel is an anatomical structure located on the anterior wrist where the hand joins the forearm. The specific architecture of the carpal tunnel serves as a passageway for several important structures between the wrist and hand. The concave floor of the tunnel is formed by the carpal bones. The flexor retinaculum—a thick, horizontal band of fascia—forms the roof. The flexor retinaculum is 3–4 centimeters wide and attaches proximally to the scaphoid tuberosity and pisiform, and distally to the trapezium and hook of the hamate. The retinaculum divides into two layers, one deep and one superficial on the radial side in order to accommodate the tendon of the flexor carpi radialis. This tendon is not considered to be contained within the carpal tunnel.
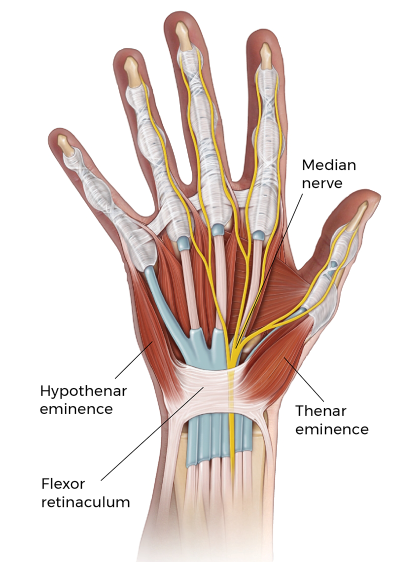
Several important soft tissues pass from the forearm to the hand through the carpal tunnel.
These include the four tendons of the flexor digitorum profundus, the four tendons of the flexor digitorum superficialis, and a single tendon of the flexor pollicis longus. The tendons of the flexor digitorum profundus and superficialis are all surrounded by a common ulnar sheath, while the flexor pollicis longus tendon is contained within a separate radial sheath.
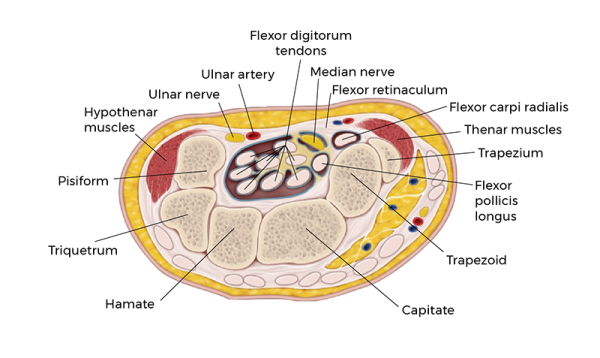
In addition to the nine tendons, the median nerve is contained within the carpal tunnel and runs between the tendons of the flexor digitorum profundus and the flexor digitorum superficialis. This peripheral nerve originates at the brachial plexus in the axilla, travels distally just lateral to the brachial artery, and crosses the artery medially halfway down the arm. The nerve then enters the anterior compartment of the forearm at the cubital fossa and follows the flexor digitorum muscles down the forearm to the carpal tunnel.
The median nerve has both sensory and motor fibers in the hand. Sensory function includes the innervation of the lateral aspect of the palm via the palmar cutaneous branch and the lateral three and a half fingers on the palmar surface of the hand via the digital cutaneous branch. Motor function includes the thenar muscles (opponens pollicis, flexor pollicis brevis, and abductor pollicis brevis) and the lateral two lumbricales in the hand.
Space within the carpal tunnel is relatively limited, and there is very little capacity for expansion due to the rigid nature of its bordering tissues. Space can be further restricted through tendon hypertrophy, increased fascial density, or fluid accumulation associated with inflammation. Carpal tunnel syndrome is a common pathology that occurs when the median nerve is compressed within the carpal tunnel.
This is characterized by pain, numbness, and tingling in the associated areas of the hand and arm, as well as atrophy in the thenar eminence and lateral lumbricales of the hand. Nerve dysfunction is often progressive and can become permanent if left untreated. Soft-tissue manipulation of the flexor retinaculum is a valuable part of treatment and prevention of carpal tunnel syndrome.
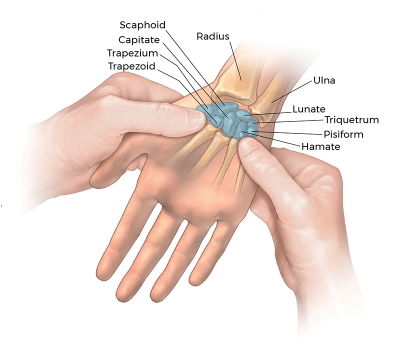
Palpating the Carpal Tunnel

Positioning: client seated or supine.
- Sit or stand at the client’s side. Gently grasp their open hand facing palm up.
- Using the pads of your thumbs, locate the thenar and hypothenar eminence of the palm.
- Moving toward the center of the palm, palpate deeply and between the soft tissue of the two eminences to locate the concave palmar surfaces of the carpal bones.
- Use special attention to locate the prominent hook of the hamate and pisiform medially, and the tubercles of the scaphoid and trapezium laterally.
Passive Stretching of the Flexor Retinaculum
Positioning: client seated or supine.
- Gently grasp and support the client’s wrist with their palm facing up.
- Firmly pin the flexor retinaculum with your thumb using cross-fiber pressure rather than compressing the carpal tunnel.
- Passively extend and abduct the thumb and fingers to elongate and free the fibers of the flexor retinaculum.
- Repeat as you pin the retinaculum in various directions.


