





The thoracic spine is a unique and often overlooked body region that plays a central role in postural alignment, respiration, and spinal mechanics. Comprised of 12 vertebrae, it serves as the axis of the rib cage and a bridge between the cervical and lumbar spine.
The rib cage forms around the central structural column created by the thoracic spine (Image 1). Each rib attaches to the thoracic vertebrae posteriorly through the costovertebral joints. In addition, the tubercles of ribs 1–10 articulate with the transverse processes of the thoracic vertebra at the costotransverse joints.

When the thoracic region is functioning optimally, the ribs move like springs, allowing the expansion and contraction of the thoracic cavity. During inhalation, the heads of the ribs rotate posteriorly and slightly superiorly on the vertebral bodies at the costovertebral joints. At the same time, the tubercles of the ribs glide along the facets of the transverse processes, permitting the angular lift of the ribs outward and upward. During exhalation, the ribs return to their resting position by reversing these motions.
The natural, kyphotic curvature of the thoracic spine is a structural adaptation that enhances shock absorption and force transmission between the upper and lower body. A functional thoracic spine allows the head and neck to rest in neutral alignment and absorbs and diffuses the load of head and arm movements. When healthy, the thoracic spine reduces strain on the cervical vertebrae, discs, and musculature.
Most trunk rotation occurs in the mid to upper segments of the thoracic spine. The lumbar spine is designed for bearing weight and flexion-extension but is not well-suited to excessive rotation. When the thoracic spine is mobile and aligned, it handles the bulk of rotation, shares movement loads, and buffers the forces moving up and down the spine.
Thoracic Spine Dysfunction
Any disruption in the mechanics of the thoracic spine has a ripple effect on the entire spine and respiratory system. When thoracic movement becomes limited or asymmetrical, the cervical spine must compensate with excessive mobility or sustained muscular effort to maintain head position and visual orientation. Similarly, the lumbar spine may begin to over-rotate or hyperextend to compensate for the lack of thoracic contribution to trunk motion. Even the rib cage loses its full capacity to expand and recoil, which restricts the effectiveness of diaphragmatic breathing. These compensatory patterns place the body under continual strain, reinforcing dysfunction and contributing to pain, fatigue, and diminished performance.
Forward-head posture is one of the most pervasive contributors to thoracic spine dysfunction. The use of technology, long hours of sitting, and poor ergonomics promote slumped posture repeated for long periods, which may result in postural distortions that become semi-permanent without corrective interventions.
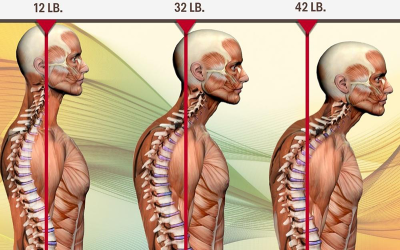
Erik Dalton described the “42-pound head” to illustrate the increased mechanical load resulting from forward-head posture (Image 2). The average adult human head weighs between 10 and 12 pounds. When the head is aligned directly over the shoulders, the spine supports it efficiently and muscular effort is minimal. For every inch the head moves forward in front of the body’s midline, the effective weight of the head increases due to the force of gravity acting further from the spine. At 2 inches forward, the head “weighs” about 30 pounds. At 3–4 inches forward, the head can exert 40–50 pounds of force on the neck and thoracic structures.
Often, therapists focus on the cervical region but forget the impact of forward-head posture on the thoracic spine, which compensates by increasing kyphosis to support the shifted head and neck. This adaptation compresses the anterior intervertebral discs, restricts facet joint mobility, and collapses the rib cage, limiting respiration. The thoracic extensors, like the erector spinae, become overstretched and weak, while anterior chest muscles like the pectoralis minor tighten. Increased kyphosis pulls the shoulder girdle anteriorly and inferiorly, leading to scapular protraction and the potential for impingement syndromes.
As diaphragmatic breathing diminishes, the body compensates by recruiting accessory respiration muscles, such as the scalenes and sternocleidomastoid muscles. These muscles are not designed for sustained breathing effort. Their overuse further reinforces forward-head posture and introduces chronic tension into the neck and upper back.
Additionally, rib fixations can trigger protective muscle guarding. The intercostal muscles, serratus anterior, spinalis thoracis, and even deeper muscles like the levator costarum can become hypertonic. This tension may contribute to pain patterns that mimic visceral dysfunction or radiate along the intercostal spaces.
Applying Myofascial Alignment Techniques
Understanding the interplay between thoracic spine alignment, rib mobility, and respiration is essential for therapists working with musculoskeletal dysfunction. Every breath we take moves the ribs and thoracic spine, and any postural distortion alters this movement. The myoskeletal alignment techniques included here are three of Dalton’s favorites for restoring the thoracic spine’s dynamic role in posture and breathing. Add these techniques to your back massage to create a more resilient and adaptable thoracic structure supporting better movement, deeper breathing, and improved overall function.
Texas Twister
Stand on the left side of your prone client. With your left hand, contact the client’s ipsilateral erector spinae muscles with your fingers facing inferiorly. Place your right thenar eminence on the contralateral erector spinae muscles. With your elbows slightly extended, drop your body weight into the tissue, creating a counterforce across the spine (Image 3). Apply a twisting and sliding motion across the musculofascial layers while maintaining downward pressure. Move your hands to a new place on the thoracic spine and repeat this technique several times. Cover the entire region with the technique.

Ask the client to bring their hands into a cuffed position behind their back to tighten some of the muscle fibers you will activate (Image 4). This practice places some stretch on the muscle spindles and enhances the effect of this technique. Using your extended finger pads or soft fists, apply a fast-paced oscillating maneuver over the rhomboids, lower traps, and erector muscles for two minutes. Again, work across the grain of the muscles and use slow inhalation and exhalation to enhance your results.

Rib Springing
With the client lying on their right side, stand behind them at their hips. Ask the client to reach over their head and grasp the top of the massage table with their left hand (Image 5). Place the web between your thumb and index finger on the ribs toward the side of the body. Push superiorly with gentle rhythmic compressions to mobilize the ribs. Ask the client to take deep breaths to increase the effect of this technique.

Conclusion
These techniques can improve the function of the thoracic spine, contributing to the body’s structural integrity, fluid movement, and ease of breath. By incorporating techniques like the Texas twister, thoracic activation, and rib springing, we can help restore healthy movement patterns and support our clients in reclaiming postural ease and respiratory freedom.


